
 By Anshu Jindal, COO, MyMipsScore
By Anshu Jindal, COO, MyMipsScore
Twitter: @MyMipsScore
This past Easter, as I watched a fellow shopper carefully picking out a basket and the Easter eggs to fill it with, I wished it was that simple for MIPS eligible clinicians to decide which quality measures to pick and which submission method to use. But it’s not. All the selected measures would have to go in one submission method basket, and when you have to put all your eggs in one basket, you got to pick that basket very carefully.
Why is submission method so important for Quality?
Quality Carries 60% or More Weight. The Quality category makes up 60% or more of your MIPS Score. If you claim ACI exclusion, then the weight for ACI category (25%) is transferred to Quality category, making the Quality category worth 85% of your MIPS score. It definitely deserves close attention.
One Submission Method per Performance Category. Although you have the flexibility to pick a separate submission method for each performance category, you can only use only one submission method for each category. Chose wisely as the benchmarks for a single measure differ based on the submission method.
Available Submission Methods
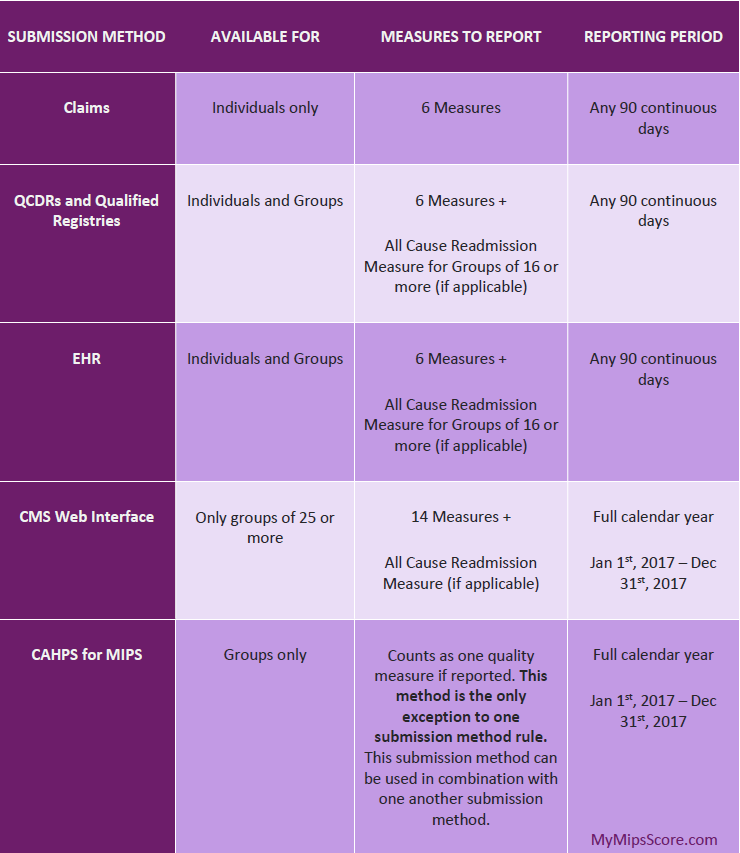
There are a five submission methods options available – Claims, EHRs, Qualified Clinical Data Registries (QCDRs)/Qualified Registries, CMS Web Interface, and CAHPS for MIPS. You would notice that QCDRs and Qualified Registries have been grouped together because CMS has defined a single set of benchmarks for all the measures available for reporting via QCDRs and Registries. However, availability and requirements of these submission methods differ a little bit.
Reporting Entity. Eligible clinicians could either report as individuals or as group using the corresponding TIN/NPI. Claims submission method is available to only clinicians reporting as individuals, whereas CMS Web Interface is only available to groups of 25 or more clinicians. Additionally, CAHPS for MIPS survey is only available to clinicians reporting as groups. To be able to use CMS Web Interface and CHAPS for MIPS for 2017, you would need to register as a group with CMS before June 30th, 2017.
Reporting Period. If you choose to submit data for quality category via CMS Web Interface or CAHPS for MIPS survey, you would have to report data for the full calendar year 2017 (Jan 1, 2017 – Dec 31, 2017). The 90-days reporting option is not available for these submission methods.
Number of Measures. Most of the providers will need to report 6 quality measures for a minimum of 90 continuous days within the calendar year. But if your specialty set has less than six measures available, you can report all the measures in the applicable specialty set without negatively impacting your score. On the other hand, if a practice chooses to use CMS Web Interface submission method (only available to groups of 25 or more), the practice would need to report all the 14 measures included in the CMS Web Interface and additional All Cause Readmission Measure if applicable. Not doing so will incur penalty.
Exception to One Submission Method Rule. This exception applies only to entities reporting as groups. The only case when groups can use two submission methods for quality performance category is when they choose to report one quality measure using CAHPS for MIPS Survey via a CMS approved survey vendor. The survey counts as one quality measure, and can be used in conjunction with any other submission method that a group is using to submit the rest of the quality measures.
Submission Methods Available For 2017
Digging Deeper Into Submission Methods
Benchmark Source for Different Submission Methods. CMS has released all the available benchmarks for quality measures that are finalized for the 2017 performance year for each applicable submission method. The benchmarks were determined based on the actual performance data submitted to PQRS in 2015, except for CAHPS and CMS Web Interface. Benchmarks for CAHPS are based on two sets of surveys: 2015 CAHPS for PQRS and CAHPS for ACOs, while CMS Web Interface utilizes Shared Savings Program benchmarks. Although the benchmark for All Cause Hospital Readmission measure is not available yet, CMS has promised to make it available in 2017. Given the diverse origin of the benchmarks, it is very logical that these benchmarks vary across different submission methods, resulting in different scores.
Measures Without Benchmarks. MIPS is a confluence of some old programs (PQRS, Meaningful Use and Value-Based-Modifiers) and some new ideas. There are many measures that don’t translate seamlessly from one submission method to the other. As a result, many measures don’t have a current benchmark for one or more submission methods. For those measures, CMS will attempt to calculate benchmarks based on 2017 performance data. Certain criteria have to be met to facilitate the creation of the benchmarks though. At least 20 reporting clinicians or groups must report that measure and in doing so, they must meet the minimum case volume of 20 patients for the reported measure; meet the data completeness criteria for that measure; have performance greater than 0% (less than 100% for an inverse measure).
If no benchmark can be calculated based on 2017 performance data, then only 3 points could be earned for that measure. The availability/non-availability of the benchmark will not become known until after March 2018, the end of reporting period for performance year 2017. Thus, it might be a good idea to report 6 measures with benchmarks that yield more than 3 points for you and additional measures without benchmarks. This way, if the new benchmarks are created and you end up earning more points on measures with newly defined benchmarks, your MIPS score will only get better.
Topped Out Measures. According to CMS, “A measure may be considered topped out if measure performance is so high and unvarying that meaningful distinctions and improvement in 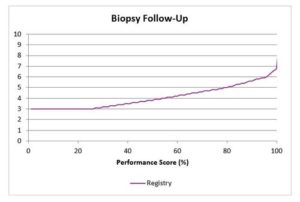 performance can no longer be made”. In simple terms, this means that at least half of the clinicians reporting that measure have performance rate of 95% or higher (5% or lower for inverse measures). You can still earn maximum score of 10 points for that measure, but you need to be at 100% performance (or 0% for inverse measures). For instance, a performance of 99.9% might only yield 6.99 points. The score will jump to 10 points only at 100% performance rate. There is no gradual increase in the score with increase in performance. CMS will gradually replace such measures with more statistically meaningful measures. The graph explains it much more clearly.
performance can no longer be made”. In simple terms, this means that at least half of the clinicians reporting that measure have performance rate of 95% or higher (5% or lower for inverse measures). You can still earn maximum score of 10 points for that measure, but you need to be at 100% performance (or 0% for inverse measures). For instance, a performance of 99.9% might only yield 6.99 points. The score will jump to 10 points only at 100% performance rate. There is no gradual increase in the score with increase in performance. CMS will gradually replace such measures with more statistically meaningful measures. The graph explains it much more clearly.
Measures Available for Submission Methods
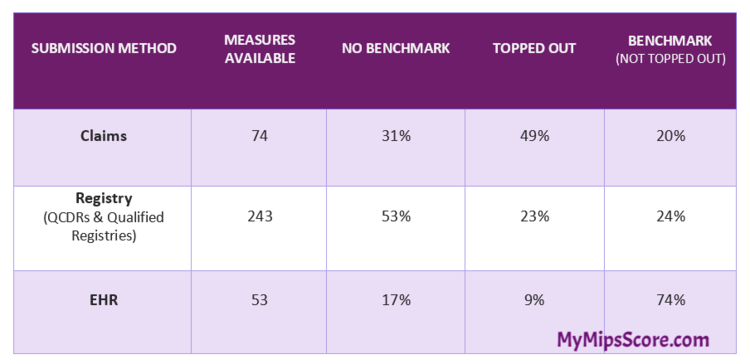
Let’s take a closer look at Claims, Registry and EHR as using these submission methods affords you the freedom to select any 6 measures that make most sense for your practice. If you report less than 6 measures (except when your chosen specialty set has less than 6 measures), your score would be impacted negatively. On the other hand, if you report more than 6 measures, only 6 measures that yield the highest score for you will be used by CMS to calculate your MIPS score.
Although each submission method offers some unique advantages, the winning combination of measures and submission method would be different for each practice (reporting entity). The decision of picking a submission method should not be driven by only the number of measures available, or by the options offered by your EHR vendor, or by your organization’s traditional reporting method of choice. That might not be in your best interest as evident from the table below.
Measure Summary for Claims, Registry, and EHR
Which Submission Method?
So, the question remains – What is best submission method for you? The best answer is (you will hate me for saying this) – it depends.
It depends on:
- The measures you pick
- The benchmarks (availability/non-availability) for selected measures for selected submission method
- Whether a measure is topped out or not
- Performance rate for the selected measures
- The bonus eligibility of chosen measures (Outcome, High Priority, and Patient experience measures earn you additional bonus points)
- If you meet end-to-end reporting bonus requirements or not.
Don’t let all the variables intimidate you. We have a solution for you. MyMipsScore™ has all the criteria for submission methods and benchmarks built-in for each measure. It enables measure analysis and score comparison across different submission methods to help you select the best eggs for your chosen basket.
This article was originally published on MyMipsScore and is republished here with permission.