
 By Rod Baird
By Rod Baird
Twitter: @rod99309
This post analyzes how regulatory changes embodied in the 2016 Fee Schedule affect LTPAC Medical Groups. The title is an accurate synopsis. Only those who believe suffering builds character will find comfort in 2016.
Back in April, a Whitehouse press release celebrated the passage of MACRA (The Medicare Access and CHIP Reauthorization Act): “At last, the doctors who care for seniors and many Americans with disabilities will no longer have to worry that about the possibility of an arbitrary cut in their pay.”
The Fee Schedule is the acid test for Physician pay; those values are now available. Nearly every medical professional billing to Medicare Part B was adversely affected. Medscape published a concise analysis of the generalized pain. The Kaiser Foundation opined on the sunsetting of the Primary Care Incentive Payments, a particularly painful cut for LTPAC Medical groups where up to 90%+ of patients receive PCIP eligible Part B services. On average, the demise of PCIP will relate to about 5%, or greater, reduction in a Group’s income. Because that payment was a ‘bonus payment’ it only applied to the Part B reimbursements which are @ 80% of the fee schedule (i.e. 8% added $s).
MACRA: proof that Life imitates Art. Giant Crustacea colonize Earth, humans are invited for lunch! You can pretend to be Dr. Who in this choose your own adventure novel. Or you might be a real Doctor subjected to MACRA – The Medicare Access and CHIP Reauthorization Act of 2015. That law promised an annual +0.5% upward Part B payment adjustment.
The Fee Schedule contained a painful surprise. Other current laws obligate CMS to find an annual Part B savings of 1% though reducing ‘potentially misvalued’ CPT®/HCPCS codes. In the past, savings came from surgery, imaging, testing, and cardiology. In 2016, CMS searched for problematic codes – the cupboard was bare! Their savings only amounted to 0.23%. That meant the remaining 0.77% had to be recovered via an across the board cut in the fee schedule. The combined results yielded an additional 0.3% cut in the fee schedule.
Hold on for more hidden cuts! – We aren’t finished exploring how LTPAC Medicine is subject to ‘Arbitrary Cuts’. Long time readers will recall my posts about possible pay cuts from Value Based Purchasing’s cost measures. This arises from the high costs the CMS attributed to LTPAC Groups due to their Patient Panel.
AMDA, and other commenters, petitioned CMS to adjust their cost benchmarks for the LTPAC Population with its high incidence of prior hospitalizations, cognitive impairment, and traumatic accidents. These efforts have included multiple face-to-face meetings, and timely written comments at each regulatory opportunity.
To summarize the CMS’ non-response “After consideration of the comments received, we will continue to work with stakeholders to further explore options for risk stratified comparisons.” In other words – the CMS chose to ignore their punitive treatment of Physician-led LTPAC medical groups. [Note – through a quirk in the phase-in of VBP risk-sharing, Medical Groups without Physicians will avoid the high cost designation in 2016 because no patients are ‘attributed’ to their TIN/NPI combinations.]
The CMS’ failure to correct its cost allocation/assignment methodologies will assign larger physician-led LTPAC Medical Groups (over 9 staff) to the ‘High Cost’ tier under the VBP stratification methodology. The bottom line – an additional 2% pay reduction to CY 2018 Part B payments.
CJR research generates more ‘proof’ that SNF Admissions are extraordinarily costly. (CJR is Medicare’s new acronym for Comprehensive Care for Joint Replacement). All recent efforts to prove the high cost of the Patients attributed to LTPAC Medical Groups used supplemental QRUR report data. Is there an independent source that shows how patients sent to SNF settings are systematically ‘high cost’? This is important because if the patient is ‘high cost’ prior to their 1st encounter with the LTPAC Physician – how can that clinician be assigned responsibility?
For years we’ve worked closely with DHG (Dixon, Hughes, Goodman), the Southeast’s largest CPA groups. In November, Michael Wolford, a Manager in DHG’s healthcare group led a presentation on the final CJR rules. DHG’s webinar, intended largely for Hospital consumption, illustrated how to analyze discharges with DRGs covered by the CJR. They included the following slide – which graphically illustrates that SNFs receive the most costly patients:
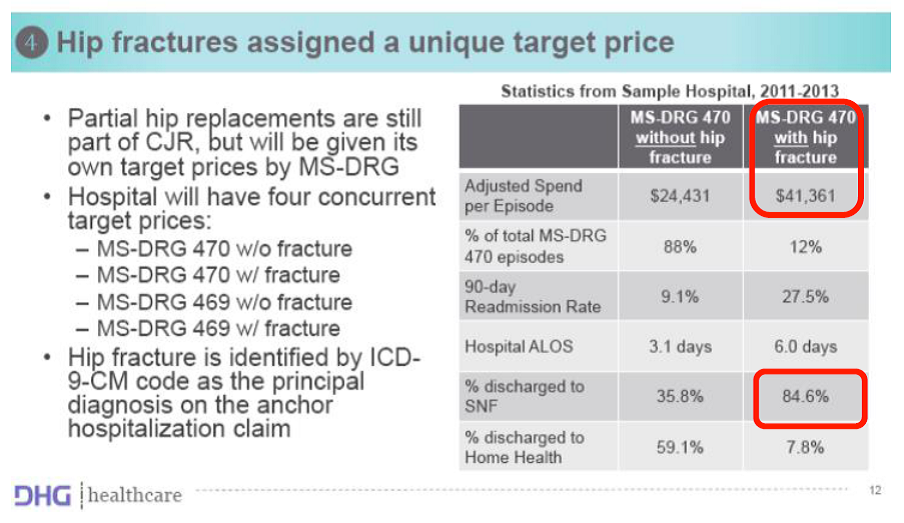 Only a small percent of all hip replacements are associated with a preceding Hip Fracture – but the costs are 76% higher. Nearly 85% of these very high cost patients are sent to a SNF. Only 36% of the (relatively)) lower cost joint replacement patients without a Hip Fracture are sent to the SNF. Note that neither the joint replacement, nor the underlying hip fracture add ‘acuity’ to the patient’s expected cost. Acuity measurement is intended to correct (normalize) the costs associated with medically complex patients.
Only a small percent of all hip replacements are associated with a preceding Hip Fracture – but the costs are 76% higher. Nearly 85% of these very high cost patients are sent to a SNF. Only 36% of the (relatively)) lower cost joint replacement patients without a Hip Fracture are sent to the SNF. Note that neither the joint replacement, nor the underlying hip fracture add ‘acuity’ to the patient’s expected cost. Acuity measurement is intended to correct (normalize) the costs associated with medically complex patients.
VBP Costs are attributed to PCPs based on measuring which Medical Group provided the most care. Assuming the physician who admits the patient provides the ‘plurality’ of all Evaluation & Management encounters, he or she becomes responsible for the entire year’s cost under Value Based Purchasing. When asked to comment on this, CMS responded:
“We noted that high costs within the post-acute and long-term care settings present a unique opportunity for these professionals to improve performance on cost and quality measures.”
This idiocy will only increase the difficulty groups face recruiting new providers to replace those retiring in the coming years.
Summarizing the Pain: the typical LTPAC Medical group should budget for at least 5.3% pay reduction in 2016, everything else remaining equal. These same groups appear predestined to suffer at least a 2% additional Part B fee reduction in CY 2018 based on ‘high cost’ status.
The math:

P.S. groups that failed to satisfactorily report PQRS in 2014 already have an additional 2016 Part B payment reduction of 2%.
The News Isn’t All Bad! There are some new regulations embodied in the updated Fee Schedule that are good – but they fix issues that should never have been problems in the first place.
CMS Approves Advanced Care Planning (ACP): All of us probably remember Sarah Palin’s Death Panels from the 2008 Presidential Campaign. That’s when CMS first proposed adding an ACP benefit to Medicare. This year, a reprise of that same concept generated surprisingly little organized protest – at least not enough to derail the inclusion of CPT codes 99497 and 99498 on the list of Covered Services.
As a symbolic issue, adding these codes is a major step towards a more intentional process for anticipating issues in End of Life Care. Yet, when I analyzed their utility in LTPAC Medicine, the tangible benefits are harder to identify. First, the codes are strictly Time Based (no rounding up the minutes) – 99497 requires a minimum of 30 minutes of service, and 99498 requires an additional 30 minutes. The payments, depending on location, will be approximately $85 and $75 respectively. They do permit Incident to billing according to their CPT® description, but elsewhere CMS states Incident to usage is prohibited in Institutional Settings (e.g. SNF/NF).
An option, always available to physicians providing ‘Counseling and Coordination of Care Services’ is to document that >50% of the encounter was for that purpose. That allows billing under the E&M Code which corresponds (strictly) to the time spent. For example, CPT® 99310 is listed at a 35 minute duration if billing under the Care Coordination option; the corresponding payment is approximately $135. There might be many good reasons to prefer use of ACP over E&M codes billed on the basis of Time, but they aren’t based on economics.
SNF E&M Encounters no longer considered Primary Care for ACO Attribution. This article already covered CMS’s inaction on attributing the SNF’s High Cost Patient population to Primary Care Physicians for VBP. In a similar request, many Hospitalists petitioned to have the SNF (POS 31) excluded as a Primary Care location for Patient Attribution under the ACO (Accountable Care Organization) program.
This Attribution rule caused problems for Hospitalists following patients into the SNF as a Post-Acute Care setting. Hospital Care is exempt from the definition of Primary Care under ACO regulations. When ACO regulations were first drafted, there were provisions inserted to preclude ‘gaming the system’. One concern was that PCPs might join multiple ACOs and improperly associate high cost patients with a particular ACO. The current ACO regulations restrict PCPs to association with a Single ACO – not a problem with Hospital Care since that is not considered Primary Care. Yet, if that hospitalist group followed their patients into the SNF, they ran afoul the rule – one ACO per PCP Practice.
The new rule allows physicians working in SNFs (POS 31) to treat patients in multiple ACOs without affecting the patients’ ACO Attribution. This revision may change care practices in unpredictable ways. In 2015, some ACOs did not enroll LTPAC Medical Groups, or follow their patients into the SNF setting. They knew there was a good statistical probability that the LTPAC group covering that SNF would capture some of the ACOs current population through ‘attribution’ which ‘deattributed’ the patient to the previous PCP & ACO.
A nuance to the rule change – it only applies to the SNF (POS31); NF (POS 32) is still considered a Primary Care location under ACO Attribution rules. This creates a strange dichotomy – patient Attribution under ACOs now does not align with the rules for VBP. Different PCP Medical Groups could be held accountable for the costs of the same patient, one under the ACO model, and a LTC group under the VBP scheme.
Housekeeping: A number of provisions in each year’s Fee Schedule are important but not directly impacting Group Practice management. The highlights for 2016:
TCM – Transitional Care Management Services: TCM is embodied in CPT® 99495-99496. These codes are available for use by an individual’s PCP when they are a patient moving from Institutional Care to a community setting. Some LTPAC Groups report using this code when their patients move from the SNF setting to either NF or ALF status. The code is complicated to use (same as with CCM). The Fee Schedule simplified the rules for Claims Submission – effectively establishing the occurrence (e.g. the date) of the required face-to-face E&M encounter as the ‘billable’ event in the month-long TCM service.
Quality Reporting Changes: This year’s Fee Schedule included multiple changes in Quality Reporting. This included both policy changes, and additions/deletions/updates to individual measures and measures groups. The next post in this Blog will focus on specific PQRS changes that affect LTPAC Medicine. Two high level changes are worth noting.
GPRO (Group Practice Reporting Option: Effective with performance year 2015, groups that elect GPRO will have the option to report by other methods. Previously, the GPRO election was ‘non-reversible’. That meant that once the GPRO election window closed (e.g. July 1, 2015) the group was unable to change their PQRS reporting strategy. Some groups discovered they misunderstood the GPRO requirements and were unable to complete reporting. That ‘trap’ was eliminated retroactively with the final regulation. For performance years 2015 and beyond groups are not bound by the GPRO election (see page 987 of the final rule for a lengthy discussion or wait until CMS literature is updated). For 2016, we believe this change creates an important strategic option for reporting. We’ll be covering that in our target educational offerings for EHR users.
Measuring Quality Performance Scores using ABC™ (Achievable Benchmarks of Care): How well a provider (or group) scores on quality measures is determining an increasing percentage of their reimbursement. The existing methodologies for establishing benchmarks, or performance goals, has deep flaws. These benchmarks were established based on Provider Performance – which yielded results that were widely divergent (e.g. higher performance scores) from the universe of patients’ performance. That arose because smart providers only reported on measures they performed with good results. As quality metric measurement became more pervasive, providers realized they would be compared to these ‘star performers’. The ABC™ program is supposed to derive its benchmarks from Patient level PQRS data, not Provider submitted information. The regulations don’t contain all the information needed to analyze the scope of this change, but the intent is correct – measure your patients’ achievements against other patients with similar conditions.
About the Author: Rod Baird is founder and president of Geriatric Practice Management (GPM) and gEHRiMed. Since 1977, he’s led provider and management organizations that deliver care to Medicare/Medicaid beneficiaries. He also was chosen to be a part of the Centers for Medicare and Medicaid Services’ (CMS) Innovation Advisors Program. Originally posted on LTC Management with permission to syndicate.